Reversal of the Polypharmacy-Survival Relationship in Poor Prognosis Cancer Patients
As seen at the CRUK Data Conference '24
Estimation of prognosis is vital for informing decisions around care and its value, especially in patients with poor prognosis cancer (PPC) where there is a risk of under- or over-treatment. Established risk stratification tools can be derived from routine healthcare records, allowing population-level research. A well-used example is the Charlson Comorbidity Index derived from admitted patient care episodes. As prescribing data are becoming more available, concomitant medication counts offer the potential for more accurate prognostication.
Polypharmacy, which is broadly defined as the use of multiple drugs serves as a risk measure and a proxy for comorbidity, notably with the Drug Derived Complexity Index (DDCI). An elevated DDCI is strongly linked to worse health outcomes and survival in both the general population and broader cancer populations.
The aim of this study was to quantitatively assess the relationship between DDCI, medication counts, and survival in specific PPC populations.
This was a retrospective cohort study conducted in NHS Lothian (Edinburgh Cancer Centre) included lung and upper gastrointestinal (GI) cancer patients diagnosed from 2015 to 2021, and having metastatic disease or no active anti-cancer treatment. Data, encompassing demographics, medical history, concurrent medications, and clinical outcomes were obtained from electronic health records including the Scottish Cancer Registry and Prescribing Information System. DDCI and medication counts were calculated using data from 5 years preceding cancer diagnosis. The primary outcome was overall survival from the diagnosis of PPC.
Kaplan-Meier analysis estimated survival probabilities based on DDCI quartiles and medication count categories (<5 or ≥5 medications). Multivariate Cox proportional hazard regression analysed the relationship of DDCI and medication count with the overall survival, adjusted for age, gender, metastatic status at diagnosis, and other relevant factors.
There were 3755 and 2654 patients in the lung, and upper GI cohorts respectively.
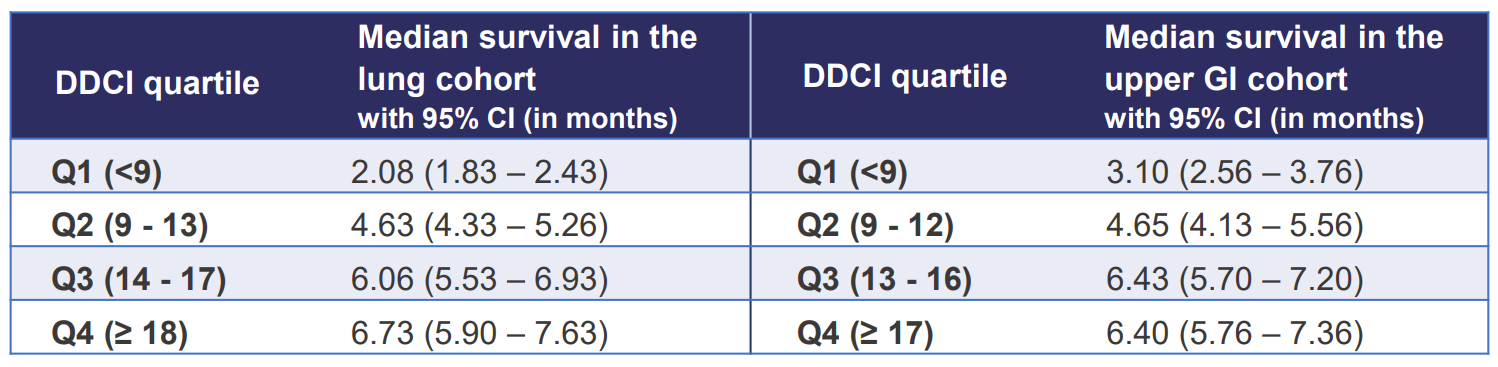
In Kaplan-Meire analysis, median survival was better with:
Higher DDCI quartiles in both PPC groups (p < 0.0001)
Similarly, with higher medication counts (≥ 5 medications) in the lung cohort
This is in contrast with wider literature, for which higher medication counts predict worse survival.
Figure 1. Median survival in DDCI quartiles in the lung and upper GI cancer cohorts.
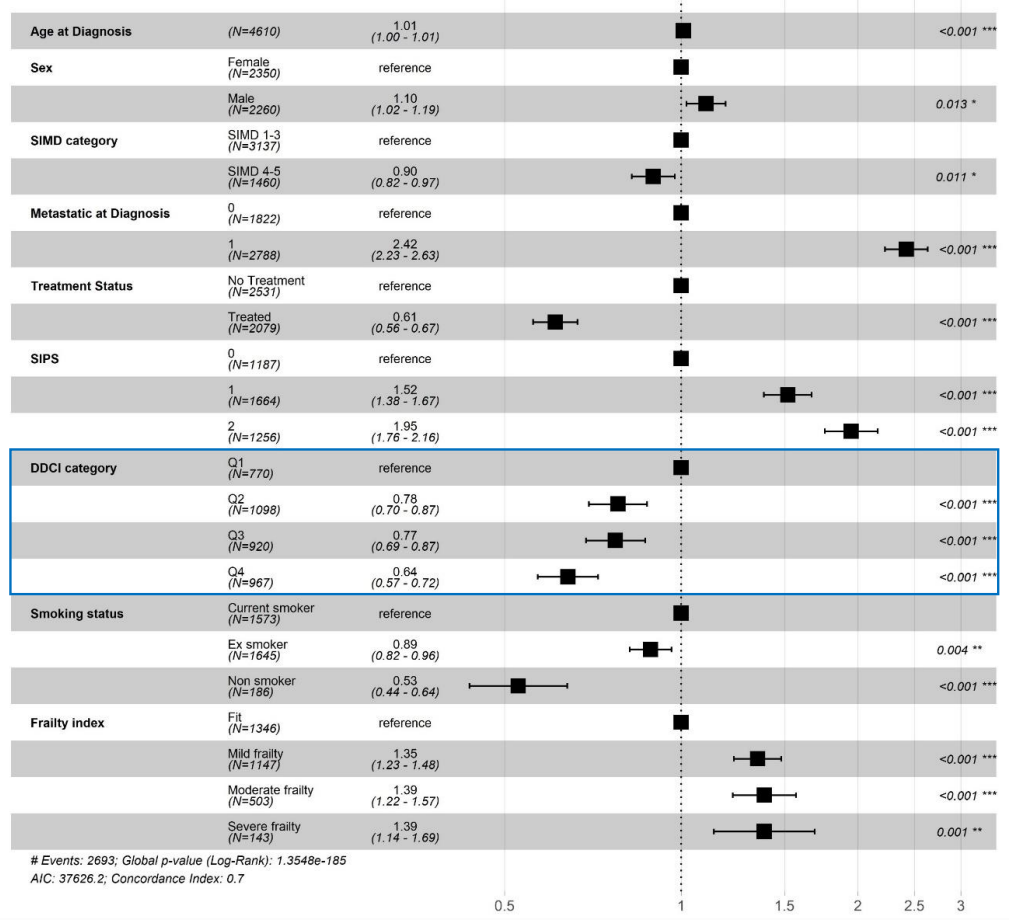
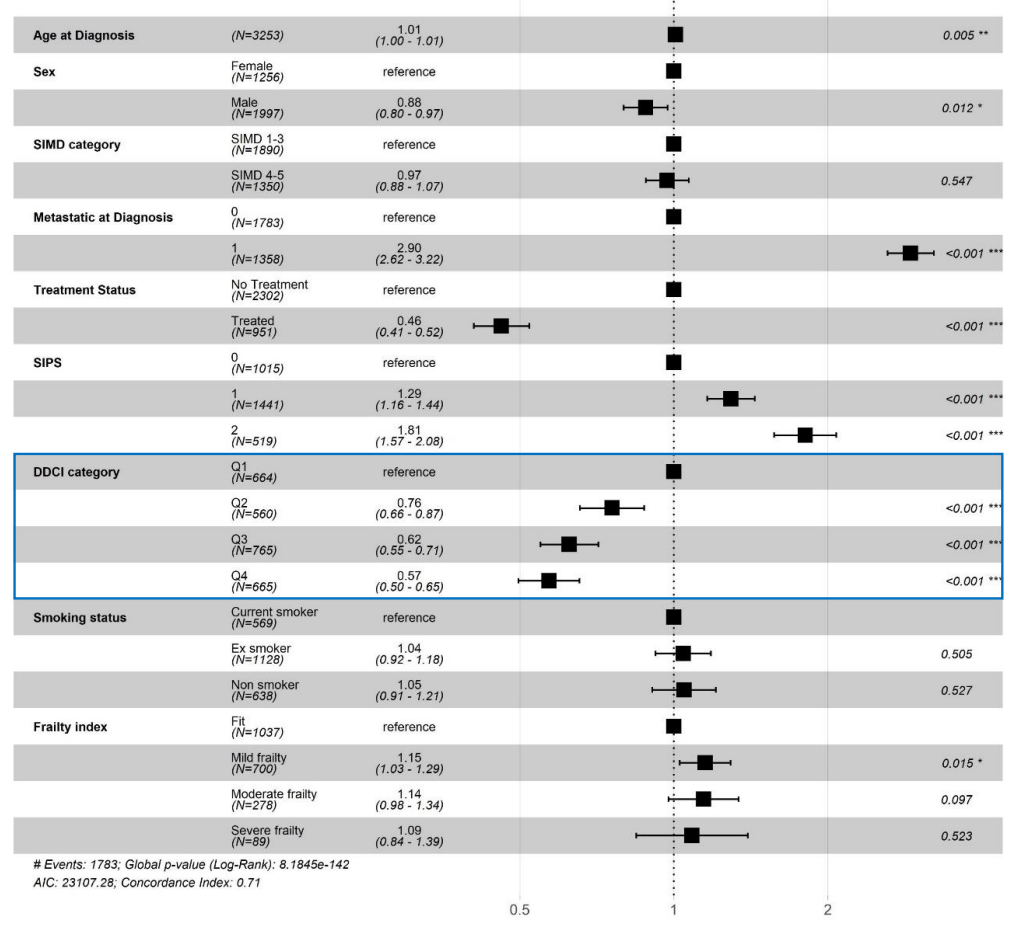
In multivariate Cox regression analysis, hazard ratios were lower in higher DDCI quartiles in lung and upper GI cohorts
Figure 2. Hazard ratios with DDCI quartiles in the lung cancer cohort.
Figure 3. Hazard ratios with DDCI quartiles in the upper GI cancer cohort.
Similarly, hazard ratios were lower with a higher medication count in both the lung and upper GI cohorts.
In conclusion, polypharmacy was predictive of better survival in specific PPC populations. These results suggest that the use of standard prognosticators in these specific populations might yield unexpected or even erroneous predictions. Further research is required to establish a potential causal link between higher medication counts and better survival in these populations.
A full copy of the project poster can be found here.
Reversal of the Polypharmacy-Survival Relationship in Poor Prognosis Cancer Patients